JAMA Facial Plast Surg. 2019 Apr 18.
Key Points
Question: Do clinical signs, such as erythema or edema, remain reliable markers of acute rejection in facial transplantation over time?
Findings: This single-center analysis of 7 patients who underwent facial transplantation with up to 8 years of follow-up demonstrated that only erythema and exanthema are reliable clinical signs with a significant association with acute rejection beyond the second posttransplant year. Subclinical rejections occurred more frequently during later follow-up times.
Meaning: Acute rejection in facial transplantation becomes less macroscopically ascertainable and accordingly more difficult to diagnose over time; thus, protocol biopsies for immune monitoring remain necessary to complement the allograft rejection diagnosis.
Authors:
Haug V, Kollar B, Obed D, Kiwanuka H, Turk M, Wo L, Tasigiorgos S, Kueckelhaus M, Riella LV, Pomahac B.
Abstract:
IMPORTANCE: Acute rejection is one of the most frequent complications in facial transplantation, with potentially severe consequences for the recipient if overlooked. Clinical signs, such as erythema or edema, are helpful to diagnose acute rejection in the early follow-up stage; however, it is not well known whether these clinical signs remain reliable markers of acute rejection beyond the second posttransplant year.
OBJECTIVE: To determine the diagnostic value of clinical signs of acute rejection after facial transplantation over time.
DESIGN, SETTING, AND PARTICIPANTS: A retrospective, single-center cohort study was conducted of patients who underwent facial transplantation at Brigham and Women’s Hospital between April 2009 and October 2014, with up to an 8-year follow-up. Medical records were reviewed until September 30, 2017. The medical records from 104 encounters with 7 patients who underwent partial or full facial transplantation were analyzed for symptoms of rejection, immunosuppressive therapy, and histopathologic findings.
MAIN OUTCOMES AND MEASURES: The occurrence of 5 clinical signs of acute rejection were evaluated: erythema, edema, exanthema, suture line erythema, and mucosal lesions. Odds ratios (ORs) were calculated to determine the statistically significant association of these signs with the histopathologic diagnosis of rejection. In addition, tacrolimus blood levels, as a surrogate marker of immunosuppressive therapy, were evaluated.
RESULTS: Of the 7 patients included in the study, 5 were men. The mean follow-up was 66 months (range, 35-101). Of 104 clinical encounters, 46 encounters (44.2%) represented rejection episodes and 58 encounters (55.8%) represented no-rejection episodes. Beyond 2 years posttransplantation, only erythema (OR, 6.53; 95% CI, 1.84-20.11; P = .004) and exanthema (OR, ∞; 95% CI, 2.2-∞; P = .004) were demonstrated to be reliable clinical signs of acute rejection in facial transplantation. There was also a statistically significant association of subtherapeutic tacrolimus levels with late rejection episodes (OR, 3.79; 95% CI, 1.25-12.88; P = .03). In addition, the occurrence of subclinical rejection was more frequent during later follow-up times (7 [24.1%] late rejections vs 1 [5.9%] early rejection). Five of 8 subclinical rejections (62.5%) were associated with subtherapeutic tacrolimus levels.
CONCLUSIONS AND RELEVANCE: Clinical signs of acute rejection in facial transplantation appear to be of limited diagnostic value, particularly after the second postoperative year. Until alternative biomarkers for rejection are identified, protocol skin biopsies will remain necessary for guiding assessments of allograft rejection.
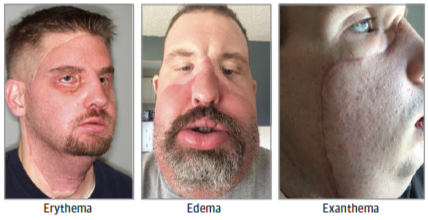
Figure 2. Typical Clinical Presentation of Signs of Acute Rejection in Facial Transplantation. Representative clinical photographs of typical signs of acute rejection in facial transplantation of erythema, edema and exanthema.