Abstract
Glomerular disease (GD) is the third leading cause of ESKD,4representing 17% of all adult kidney transplant recipients (KTRs) in the United States.5Moreover, patients with GD tend to be younger than those with other ESKD etiologies, which underscores the critical need to focus on improving long-term kidney allograft survival. Despite its impact, a significant disparity exists in the inclusion of patients with GD in clinical trials of KTRs. Owing to concerns about primary GD recurrence posttransplantation and its potential impact on trial outcomes, patients with GD may be excluded from participation. These exclusions are often based on historical and generalized assumptions, despite growing evidence supporting individualized risk stratification based on GD subtypes and phenotypic profiles. Advances in understanding the pathophysiology and recurrence risk of specific GD subtypes challenge the rationale for blanket exclusions and highlight the need for more inclusive trial designs.
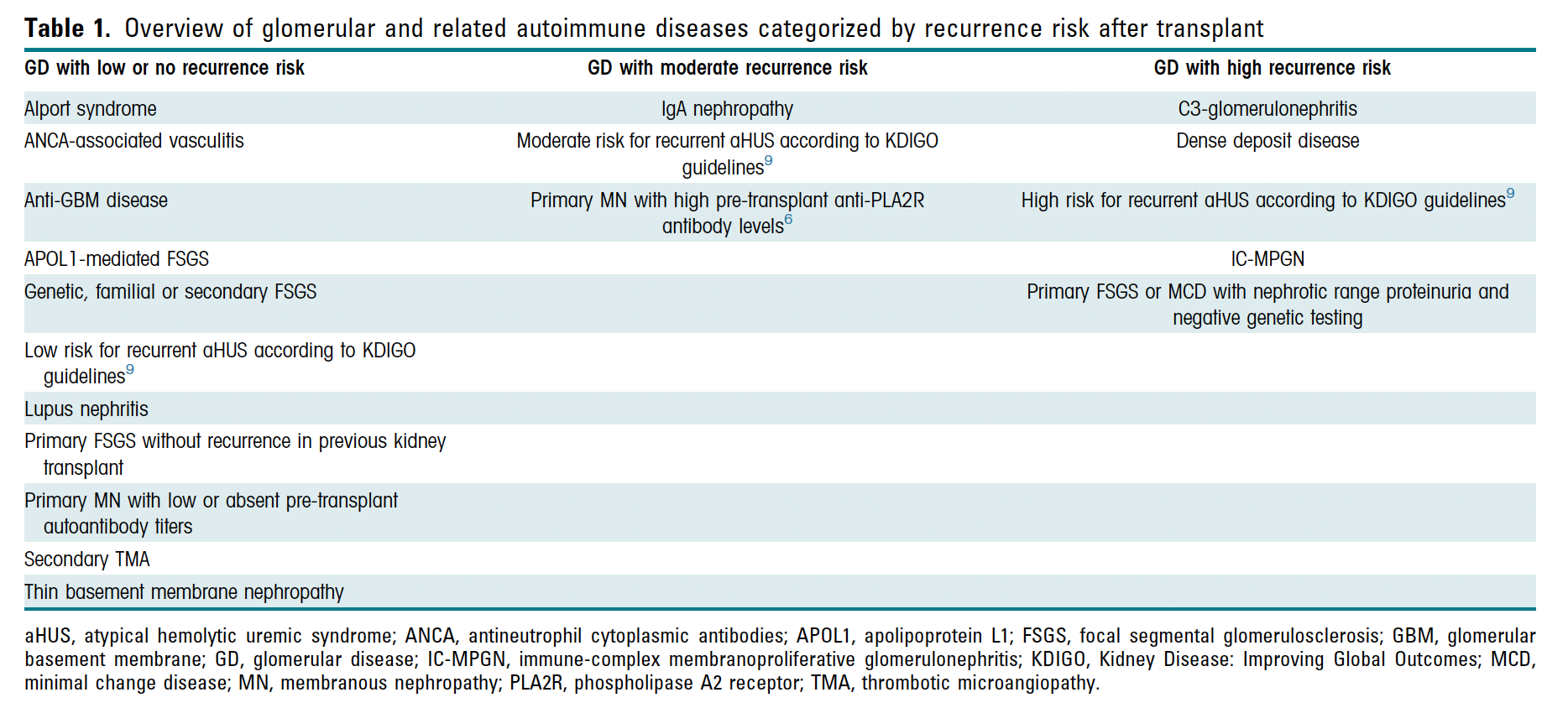
This study investigated the prevalence of excluding KTRs with primary GD from interventional clinical trials and offers guidance on recurrence risk stratification to promote equitable trial participation. By addressing these disparities, we aimed to enable evidence-based management strategies that improve outcomes for all KTRs, including those with GD.
PDF link