Authors:
Isakov O, Ghinea R, Beckerman P, Mor E, Riella LV, Hod T.
Abstract:
Background: Persistent hyperparathyroidism (pHPT) is frequently seen after transplantation contributing to post-transplant complications.
Methods: We conducted a retrospective single center analysis to explore the relationship of early pHPT and long-term allograft outcome. Patients were divided into high (N = 153) and low (N = 252) PTH groups based on serum parathyroid hormone (PTH) level 3 months post-transplant (PTH ≥ 150 and < 150 pg/mL, respectively).
Results: High PTH was found to be an independent predictor for reduced kidney allograft function up to 3 years post-transplant. eGFR decreased by 11.4 mL/min (P < .001) and the odds of having an eGFR < 60 mL/min 3 years post-transplant were sixfold higher (P < .01) in the high compared to the low PTH group. Subgroup analysis based on eGFR 1 year post-transplant, presence of slow graft function (SGF), and transplant type revealed similar results. High PTH three months post-transplant was also independently associated with an increased risk for overall mortality and for death with a functioning graft (P < .05).
Conclusions: pHPT three months post-renal transplantation is an independent predictor for a worse allograft function up to 3 years post-transplant and a risk factor for mortality. This relationship remains statistically significant after accounting for baseline allograft function, presence of SGF and serum mineral levels abnormalities.
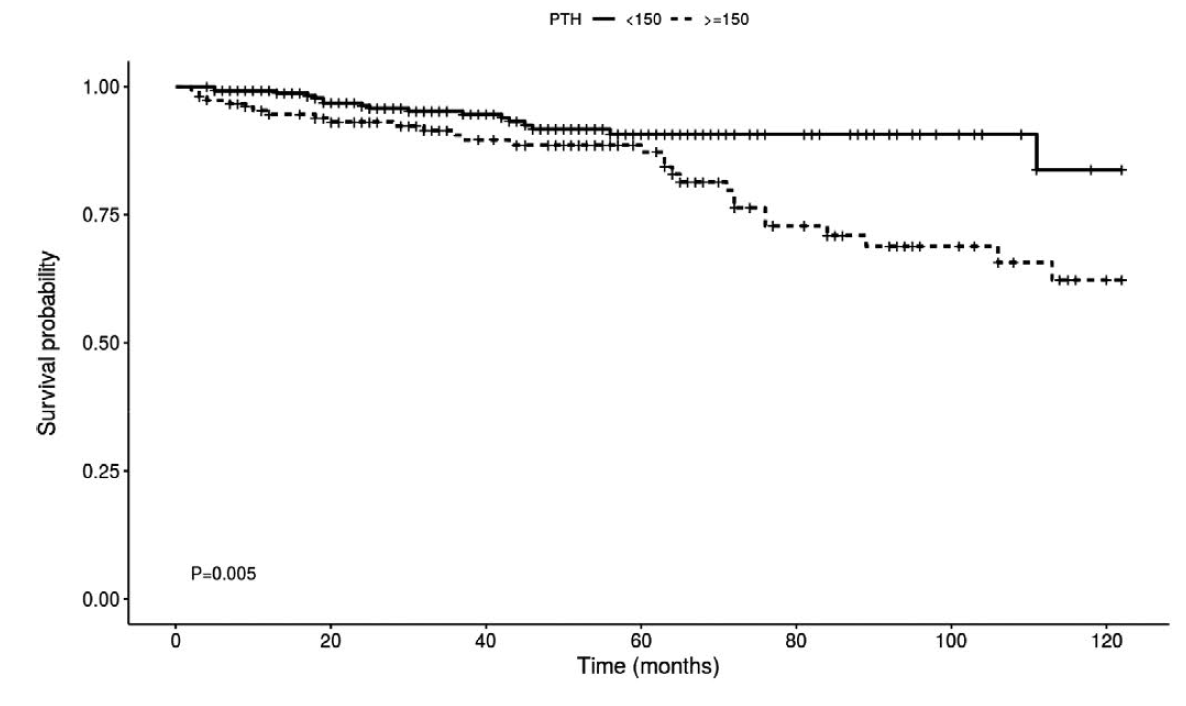
Figure:
Univariate Kaplan–Meier curves for overall survival according to PDH levels.