Transplantation. 2019 Apr 10. [Epub ahead of print]
Authors:
Leon J, Perez-Saez MJ, Batal I, Beck LH Jr, Rennke HG, Canaud G, Legendre C, Pascual J, Riella LV.
Abstract
Membranous nephropathy (MN) is a common cause of nephrotic syndrome after transplantation and is associated with an increased risk of allograft loss. MN may occur either as a recurrent or as a de novo disease. As in native kidneys, the pathophysiology of the MN recurrence is in most cases associated with anti-phospholipid A2 receptor antibodies (antiPLA2R). However, the post-transplant course has some distinct features when compared to primary MN, including a lower chance of spontaneous remission and a greater requirement for adjuvant immunosuppressive therapy to induce complete remission. Whereas the efficacy of rituximab in primary MN is now well established, no randomized studies have assessed its effectiveness in MN after transplant, and there are no specific recommendations for the management of these patients. This review aims to synthesize and update the pathophysiology of post-transplant MN, as well as to address unsolved issues specific to transplantation, including the prognostic value of antiPLA2R, the risk of living-related donation, the link between de novo MN and rejection, and different therapeutic strategies so far deployed in post-transplant MN. Lastly, we propose a management algorithm for patients with MN who are planning to receive a kidney transplant, including pre-transplant considerations, post-transplant monitoring and the clinical approach after the diagnosis of recurrence.
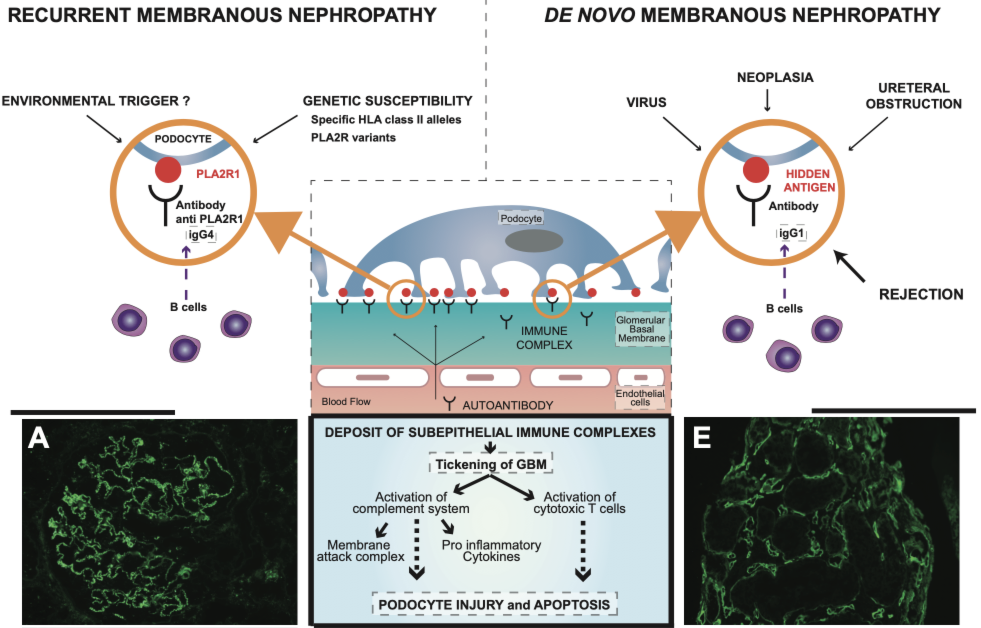
Figure 2. Pathophysiology of post-transplant membranous nephropathy.