 Nice debate on ASN Transplant Community about the use of IVIG for BK nephropathy.
Nice debate on ASN Transplant Community about the use of IVIG for BK nephropathy.
Personally, I have used IVIG in a handful of patients with refractory BK nephropathy in the past. However, I have convinced myself that there is no data supporting that.
Most case series used IVIG in combination with reduction of immunosuppression (Sener et al. Transp 2006), preventing any conclusion on the matter. We had a nice debate with Jay Fishman (MGH Transplant Infectious Disease expert) on last AST Fellow’s Symposium about this issue.
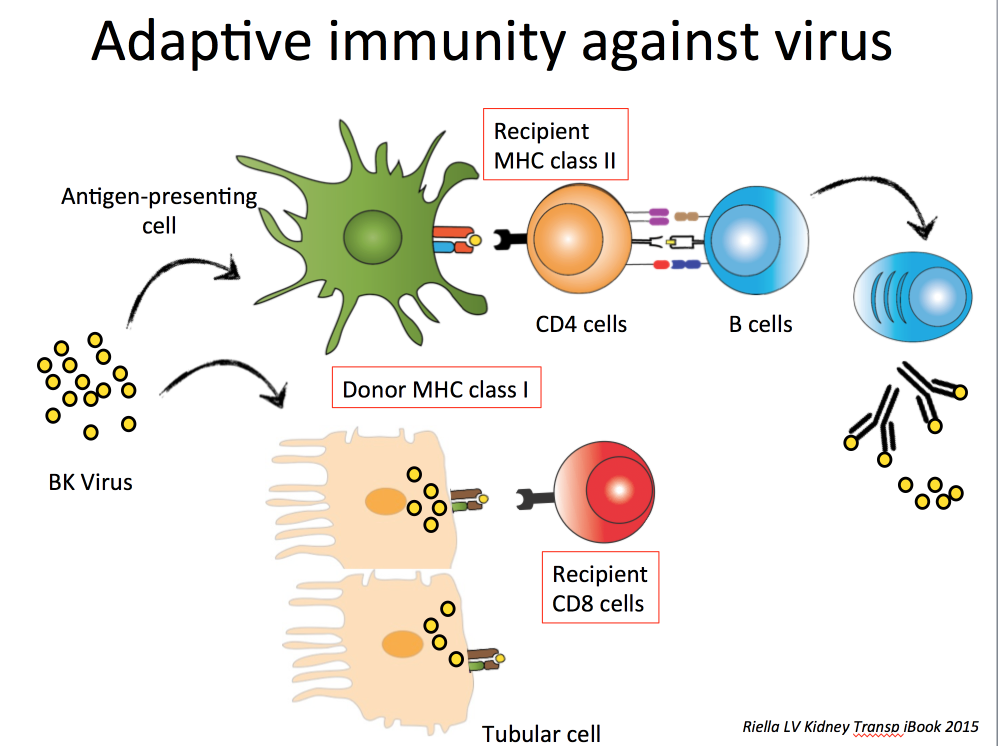
The conclusion was that an effective viral response requires cytotoxic T cells to kill infected cells (Figure above). Antibodies against the virus may help neutralize circulating virus but alone are not capable of stopping an ongoing infection. In particular, prior immunity against BK (IgG BK positive prior to transplant) does not seem to protect against post-transplant BK infection (different than CMV exposure). However, one must keep in mind that there are at least 4 different BK genotypes and immunity against one genotype does not equal immunity to all genotypes, which may explain some of the controversies on the topic (Pastrana et al. PLOS Pathogens 2012).
Overall, reduction in immunosuppression remains the cornerstone of BK viremia treatment.
Remaining controversial topics:
- Should you give steroids if intense inflammation? Some data suggest it may not be good…
- Should you stop or just reduce antiproliferative dose? Unclear on my view, but intensity of viremia and allo-immune risk must be balanced here.
- Should you switch to an mTOR inhibitor? Some interesting data suggesting that mTOR inhibitors suppress BK replication (similar to suppression to other virus like CMV) (Hirsch et al. AJT 2016)