Transplant Direct. 2019 Apr 15;5(5):e446.
Uffing A, Hidalgo LG, McMullan C, Perry J, Milford EL, Murakami N, Yeung MY, Guleria I, Wood IG, Akalin E, Azzi J, Chandraker AK, Riella LV.
Abstract:
BACKGROUND:
Many kidney transplant centers in the United States report both HLA class I and II antibodies detected by sensitive solid-phase assays (SPAs) to United Network for Organ Sharing as unacceptable antigens, significantly reducing the compatible donor organ pool and prolonging waiting time for highly sensitized patients. However, the clinical relevance of all detected donor-specific antibodies (DSAs) by SPA is not unequivocal, because fluorescence intensity does not always accurately reflect antibody pathogenicity. Our center does not exclude patients from transplantation based on DSA class II.
METHODS:
We performed a retrospective analysis in 179 deceased-donor kidney transplant recipients with solely DSA class II before transplant and patients without DSA and compared graft survival, rejection, and clinical outcomes. Patient survival was also compared with matched controls on the waiting list.
RESULTS:
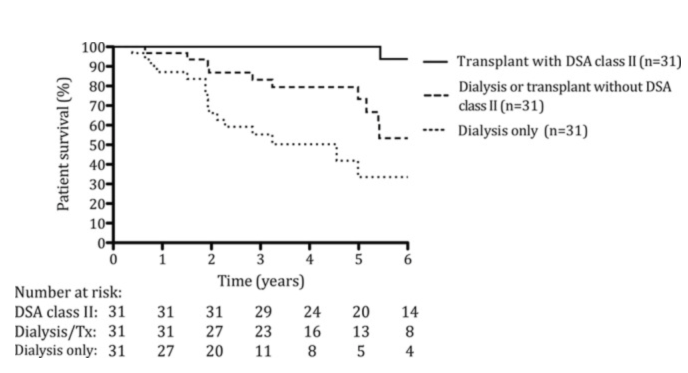
Patients transplanted with DSA class II showed a clear survival benefit compared with matched patients who remained on dialysis or were waitlisted on dialysis/transplanted at 5 years (100%, 34%, and 73%, respectively). After a mean follow-up of 5.5 years, there was no significant difference in death-censored graft survival between transplanted patients without DSA and those with preformed DSA class II (adjusted HR 1.10; 95% confidence interval, 0.41-2.97), although the incidence of rejection was higher in recipients with DSA class II (adjusted HR 5.84; 95% confidence interval, 2.58-13.23; P < 0.001). Serum creatinine levels at 1, 3, and 5 years posttransplant did not differ between groups. No predictors of rejection were found, although patients who received basiliximab induction therapy had higher incidence of rejection (100%) compared with those who received antithymocyte globulin (52%).
CONCLUSIONS:
We conclude that for highly sensitized patients, deceased-donor kidney transplantation with DSA class II yields a survival benefit over prolonged waiting time on dialysis. Instead of listing DSA class II as unacceptable antigens, an individual approach with further immunologic risk assessment is recommended.
Figure 1. Kaplan-Meier survival analysis of patients transplanted with DSA class II compared with 2 matched control groups of patients who remained on dialysis (dialysis only) or who were waitlisted on dialysis and could receive a compatible kidney transplant (dialysis or transplant). DSA, donor-specific antibody; Tx, transplant.