Front. Nephrol. 2:1047217. doi: 10.3389/fneph.2022.1047217
Authors:
Yamamoto T, Pearson DS, Ababneh EI, Harris C, Nissaisorakarn P, Mahowald G, Heher YK, Elias N, Markmann JF, Lewis GD, Riella LV.
Abstract:
Preformed donor-specific antibodies are associated with a higher risk of rejection and worse graft survival in organ transplantation. However, in heart transplantation, the risk and benefit balance between high mortality on the waiting list and graft survival may allow the acceptance of higher immunologic risk donors in broadly sensitized recipients. Transplanting donor-recipient pairs with a positive complement dependent cytotoxic (CDC) crossmatch carries the highest risk of hyperacute rejection and immediate graft loss and is usually avoided in kidney transplantation. Herein we report the first successful simultaneous heart-kidney transplant with a T- and B-cell CDC crossmatch positive donor using a combination of rituximab, intravenous immunoglobulin, plasmapheresis, bortezomib and rabbit anti-thymocyte globulin induction followed by eculizumab therapy for two months post-transplant. In the year following transplantation, both allografts maintained stable graft function (all echocardiographic left ventricular ejection fractions ≥ 65%, eGFR>60) and showed no histologic evidence of antibody-mediated rejection. In addition, the patient has not developed any severe infections including cytomegalovirus or BK virus infection. In conclusion, a multitarget immunosuppressive regimen can allow for combined heart/kidney transplantation across positive CDC crossmatches without evidence of antibody-mediated rejection or significant infection. Longer follow-up will be needed to further support this conclusion.
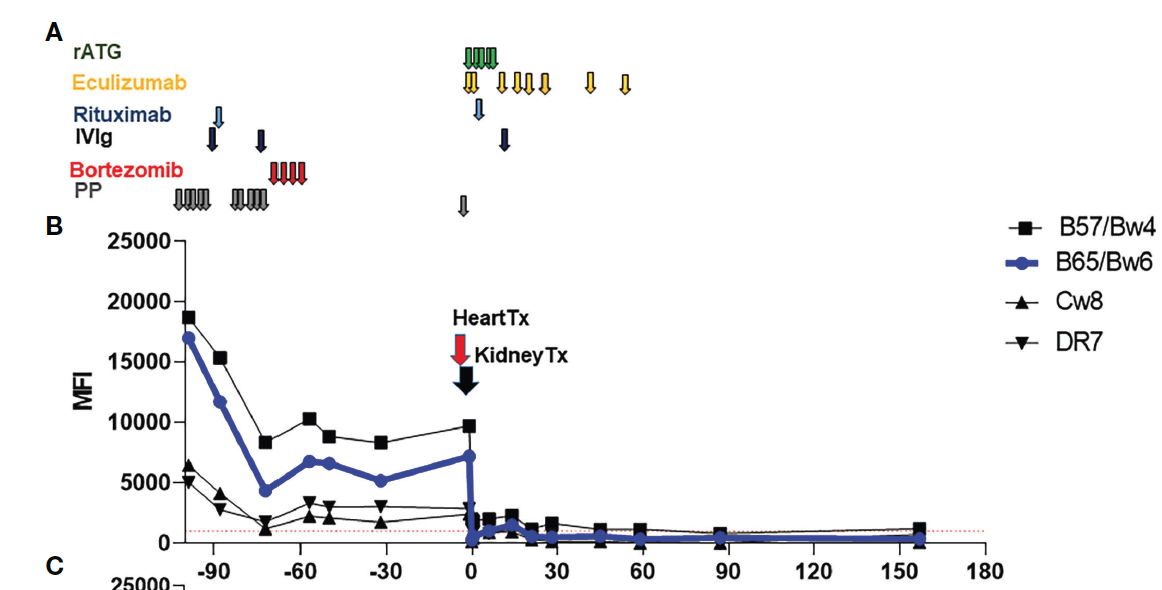
Figure: Immunosuppressive therapies and trend of donor specific antibodies (DSA). (A) Immunosuppressive therapies used pre-transplant and early post-transplant. Maintenance therapies are not depicted (tacrolimus, mycophenolate mofetil and a steroid taper.) (B) Class I and II DSA following desensitization and SHK transplantation.